Hearing loss
The type of hearing loss that your child has refers to the part of the ear that is affected.
Diagram of the ear
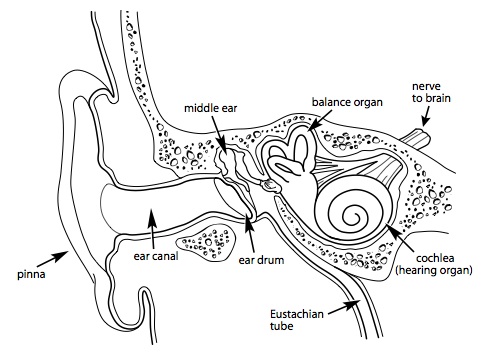
Parts of the ear
- The outer ear includes the pinna (fleshy outside part of the ear), and the ear canal. These structures collect sound and direct it towards the eardrum.
- The middle ear includes the eardrum, a space filled with air, and three small bones. These structures are responsible for conducting the sound from the outer ear to the inner ear. The Eustachian tube (normally closed) opens to equalize the air pressure in the middle ear.
- The inner ear includes the cochlea and the balance organ. The cochlea contains tens of thousands of tiny hair cells that are each tuned to different pitches. These hair cells respond to incoming sound, and pass on information to the hearing nerve.
Conductive hearing loss: Conductive loss results from a problem in the outer or middle ear, affecting the way the sound travels through the ear. A common cause of conductive hearing loss in children is
fluid in the middle ear. Middle ear fluid can sometimes get better by itself. If middle ear fluid persists, becomes infected, or causes a hearing loss, your child might need medical treatment (i.e., antibiotics or tubes). Conductive hearing loss can also be permanent, as in a malformation of the outer or middle ear (like ‘atresia’) that prevents sound from travelling through the ear. This type of hearing loss is often managed with hearing aids and/or surgery from an Ear Nose and Throat doctor as well as early intervention services.
Sensorineural hearing loss: Sensorineural hearing loss results from a problem in the cochlea. Your child may have been born with this type of hearing loss. It can also be the result of damage, disease, injury, or certain medications. Sensorineural hearing loss is almost always permanent and cannot be improved with medicine or surgery. Usually, hearing aids or other listening devices are the best treatment for sensorineural hearing loss.
Mixed hearing loss: Mixed hearing loss is a combination of conductive and sensorineural hearing loss.
Auditory Neuropathy Spectrum Disorder: Auditory neuropathy is a hearing disorder in which sound enters the inner ear normally but the transmission of signals from the inner ear to the brain is impaired.
It is important to know what kind of hearing loss your child because:
- It will help you to understand your child's hearing loss
- It will help to determine the best treatment plan for your child.
Download the
Types of Hearing Loss pamphlet (PDF) for more information.
Normal hearing sensitivity is defined as hearing at 15 dB or better. A slight hearing loss is defined as hearing sounds beginning around 20-25 dB.
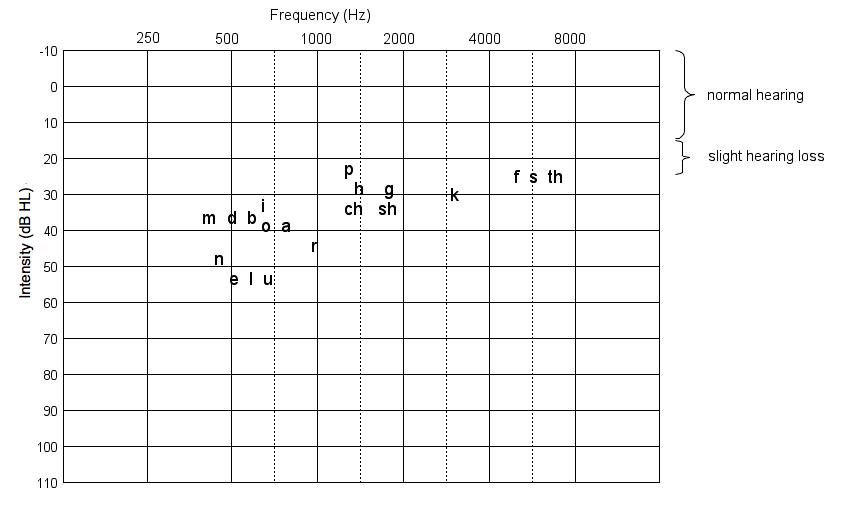
This diagram shows the range of normal hearing and slight hearing loss. The further towards the bottom of the graph, the more severe the hearing loss. A few speech sounds are also plotted, indicating the approximate frequency (pitch) and intensity (loudness) of each sound. These speech sounds are representative of speech at average loudness at close proximity and in a quiet environment.
Speech sounds differ in terms of frequency (pitch) and intensity (loudness). Vowel sounds such as 'a', 'e', 'i', 'o' and 'u', tend to be lower in frequency (pitch) and louder in intensity. Consonants such as 's', 'p', 't', 'sh', 'k', and 'f' tend to be higher in frequency (pitch) and softer in intensity. How much hearing loss your child has will determine how he or she will be able to hear normal conversational speech.
The effects of slight hearing loss are subtle, but may include difficulty in:
- hearing faint or distant speech (when a person is at a distance greater than three feet)
- hearing the fine distinctions in word sounds, such as the “s” sound in plurals, (lady vs. ladies) and possessives (Tommy vs. Tommy’s). Verb tenses might also be unclear (is vs. was, fill vs. filled).
- hearing in background noise, such as a noisy classroom or restaurant, or with the television on in the room
- following a fast-paced conversation
- picking up subtle conversational cues
- focusing on what the teacher is saying in the classroom
Your child might experience problems like these:
- Your child might have difficulty in school when the classroom is noisy or if he or she is not seated close to the teacher.
- Your child might become fatigued in school from the increased effort it takes to listen.
- Your child might respond inappropriately if he or she has missed parts of a conversation.
Some things you can do to& help your child in the classroom:
- You can make sure your child’s teacher knows about your child’s hearing loss.
- Your child should sit close to the teacher where good eye contact is possible.
- If your child has one ear that hears better, that ear should be on the side closer to the teacher.
- Your child might benefit from a Soundfield or personal FM system. In these systems, the teacher wears a microphone which transmits either to a headset worn by your child, or to speakers in the classroom. In both cases, the teacher’s voice is amplified so that it is more easily heard above the background noise of the classroom.
Download the
Slight Hearing Loss pamphlet (PDF) for more information.
How well your child will understand speech depends on the degree and configuration of hearing loss. Hearing loss is divided into categories depending on the severity.
Here are the categories of hearing loss, and how you can expect your child to hear speech.
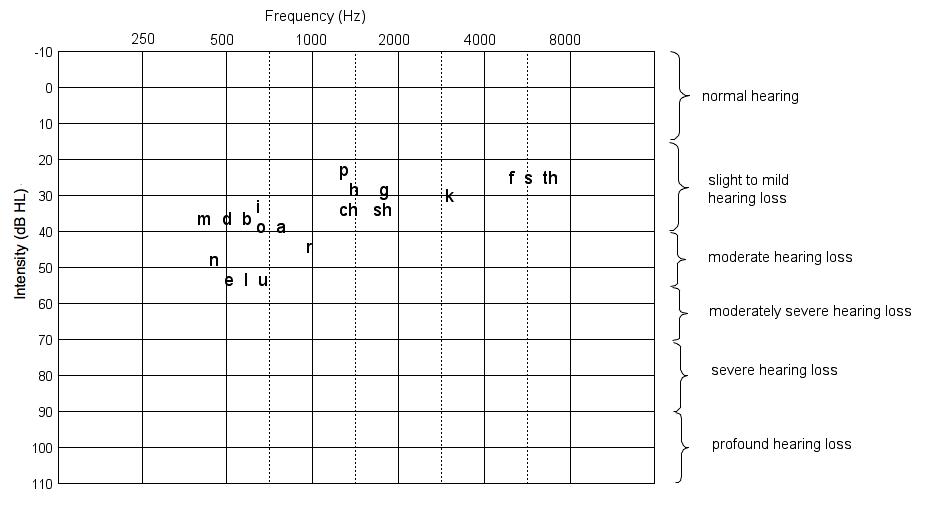
This diagram shows the categories of hearing loss - the further towards the bottom of the graph, the more severe the hearing loss. A few speech sounds are also plotted, indicating the approximate frequency (pitch) and intensity (loudness) of each sound. The speech sounds are plotted at levels of loudness if they were spoken in average conversational loudness in a quiet environment.
Speech sounds differ in terms of frequency (pitch) and intensity (loudness). Vowel sounds such as 'a', 'e', 'i', 'o' and 'u', tend to be lower in frequency (pitch) and louder in intensity. Consonants such as 's', 'p', 't', 'sh', 'k', and 'f' tend to be higher in frequency (pitch) and softer in intensity. How much hearing loss your child has will determine how he or she will be able to hear normal conversational speech.
-
Normal hearing (0-15dB): Your child will likely be able to detect and discriminate all speech sounds even at very quiet levels.
-
Slight (20-25dB) and
Mild hearing loss (25-40dB): Your child might have difficulty hearing faint or distant speech and have difficulty in group environments. Your child will likely be able to hear sounds at close distances and in quiet environments.
-
Moderate (40-55dB) and
Moderately-Severe hearing loss (55-70dB): Your child might have difficulty detecting and discriminating consonants (e.g., the s, sh, th, ch, f, k, and p sounds) and might rely on combined clues from several sounds, words, and patterns of speech to understand what is said.
-
Severe hearing loss (70-90dB): Your child might be able to identify environmental sounds; he or she might be able to discriminate vowels but will likely have difficulty discriminating consonants.
-
Profound hearing loss (90-105dB): Your child will likely only hear loud environmental sounds and feel vibrations.
Children often have hearing loss that is a combination of different levels for different pitches. An example is a
mild hearing loss in the low pitches and a
severe hearing loss in the high pitches.
Untreated hearing loss can have significant negative effects on speech and language development.
Early intervention services (or early communication support services), medical treatment and/or hearing devices can significantly minimize the negative effects of hearing loss. Use of sign language, hearing aids or other hearing devices are usually needed for permanent hearing loss.
You should work with your audiologist and other professionals to be sure to get appropriate treatment and a follow-up plan for your child’s hearing loss.
Download the
Effects of Hearing Loss pamphlet (PDF) for more information.
Approximately 2 babies in every 1000 births have a unilateral hearing loss. A newborn hearing-screening test can identify a unilateral hearing loss within the first few months of life. The test may even be given before your newborn child leaves the hospital.
There are many strategies you can use to enhance your child’s listening skills. In addition, there are specific changes that can be made to the home environment to make listening easier for your child.
A unilateral hearing loss affects your child in several ways:
-
Hearing in background noise: Important sounds, such as the speech of your child’s caregiver, are not as clear and are harder for your child to hear when there is other noise in the background.
-
Finding or localizing a sound: Most children find it difficult to tell where a sound is coming from when they do not have the same hearing in both ears.
-
Language development: Children learn to speak by saying what they hear. If your child does not hear speech clearly, it may be more difficult for your child to develop clear speech.
-
Hearing soft sounds: Soft voices and voices that are far away may be more difficult for your child to understand.
Speech and language development
Children learn to talk by listening to those around them. Some children with a unilateral hearing loss may experience some difficulties learning new words or pronouncing all words clearly. A recent study looked at children with unilateral loss at age 3 and found that only the children with severe or severe to profound unilateral loss were having difficulty. This type of outcome is similar to other research studies on the subject.
Ask your care team for some strategies that help your child to develop good listening skills. This is called auditory training.
There are some things that you can do to modify your environment so that it is easier for your child to hear you:
- Reduce or remove sources of background noise such as televisions and dishwashers. Move away from sources of noise that you can’t reduce.
- Position your child so that the ear with normal hearing is directed toward the sound you want the child to hear.
- When you are talking to your child, get close. Get even closer when you are in a noisy environment.
There are some communication strategies that you can use to ensure that your child hears you:
- Speak
clearly to your child on the side where his/her hearing is normal.
- Avoid shouting as it will actually add distortion to your speech, making it even harder to understand what you are saying.
- Rephrase rather than repeat sentences that are not understood.
- Use visual cues (facial expressions, gestures).
- Speak clearly (not too loud or too soft; not too fast or too slow).
- Use appropriate facial expressions and body language.
- Have visual aids on hand (pictures, books, toys).
- Get your child’s visual attention before speaking.
- Be sure there is good lighting when you are speaking to your child.
Amplification options:
A hearing aid may be helpful depending on the nature of your child’s hearing loss. Your audiologist will be able to tell you if a hearing aid will help your child.
For school-aged children, there are a few assistive listening devices that may be helpful. For example, sound-field or personal amplification systems can help a child to hear better in the classroom. In these systems, the teacher wears a microphone which transmits either to a headset worn by your child, or to speakers in the classroom. In both cases, the teacher’s voice is amplified so that it is more easily heard above the background noise of the classroom.
Here are some sources of health care support for your child’s hearing loss:
- Visit an otolaryngologist (ENT) if middle ear fluid or infections are present.
- Have your child’s hearing tested on a regular basis, as recommended by your audiologist.
- Arrange classroom observation and consultation with a speech and language pathologist or hearing resource teacher in your child’s school district.
- Ask your early interventionist for some strategies that help your child to develop good listening skills. This is called auditory training.
As your child’s parent, you are part of a team. Your partners are your health care provider, your audiologist, and your early interventionist who is familiar with hearing loss and auditory skill development. Your team can check to see if the unilateral hearing loss has an impact on speech and language learning.
Download the
Unilateral Hearing Loss pamphlet (PDF) for more information.
Hearing loss is a common side effect of treatment for some types of cancer. Sometimes, the disease itself can cause hearing loss.
Some of the treatments for cancer that can damage hearing include:
- chemotherapy drugs such as cisplatin
- radiation to the head or brain
- surgery involving the brain, ear, or auditory nerve
- some medications including certain antibiotics and diuretics
The Audiology Department at BC Children's Hospital monitors the hearing of children who are undergoing treatment for cancer, and provides some follow-up hearing assessments once treatment is finished.
For more information on cancer treatments and hearing loss, refer to the CureSearch website.
More information can also be found at the BC Children's Hospital Oncology, Hematology and Bone Marrow Transplant website.
Many babies with cleft palate have middle ear fluid at birth or in the newborn period. This fluid affects the baby’s hearing. By the time babies with cleft palates are 9 months old and are ready to have their palate repaired, most will have middle ear fluid and temporary hearing loss.
Why does this happen?
When a child has a cleft palate, some of the muscles that help a tiny tube in the ear to open may not function normally. This tube is called the Eustachian tube.
Many babies with a cleft palate and middle ear fluid will have surgery to put tubes in the ears to drain the fluid and help keep air in the middle ear. The tubes are placed by an Ear Nose and Throat ( ENT) doctor. Usually this surgery is done at the same time the baby is having surgery to repair the palate.
How does middle ear fluid affect my baby’s hearing?
When the middle ear is filled with fluid, the eardrum and the tiny bones in the middle ear can’t move as well as they should. It is harder for the sounds to get to the inner ear and sounds will be muffled. Put your hands over your ears to see what this might sound like.
You baby will have more trouble hearing softer sounds, and louder sounds will sound quieter.
Most babies with middle ear fluid and mild hearing loss will respond to sounds at home.
Middle ear fluid often changes . This means that your baby’s hearing can be better on some days, and worse on others.

